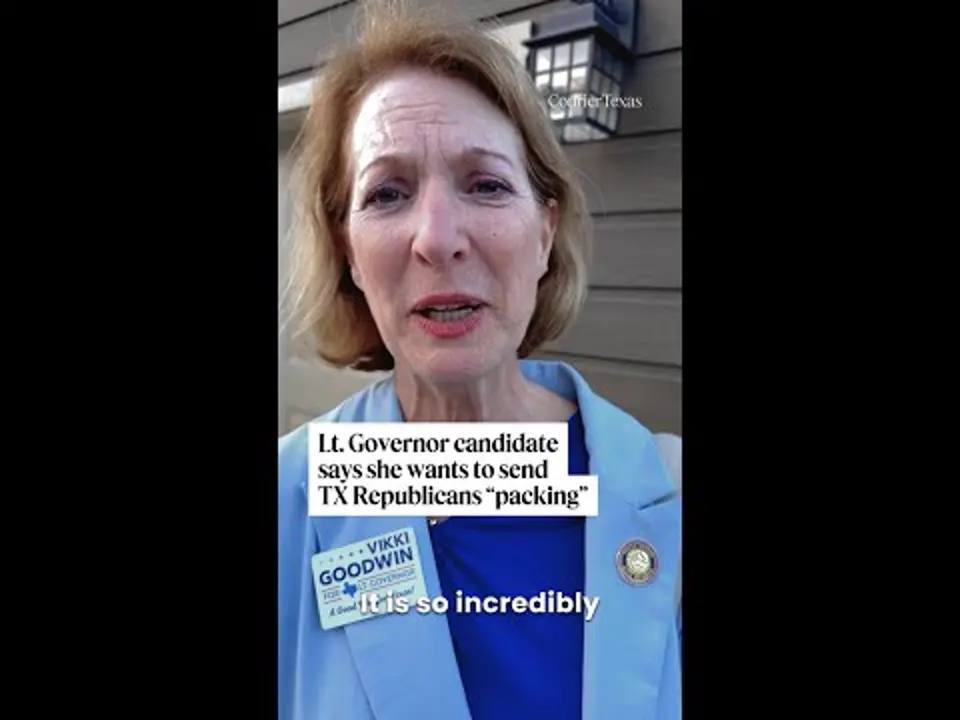
Tamika Davis, right, walks through MLK Park with three of her children, from left, Shanara, 3, Matthew, 11, and Lionel Jr., 2, in San Antonio, Thursday, May 30, 2024. As a cancer patient, she said a case manager set a book of available resources on her bedside table and did nothing else. Davis, a nursing professor, found the book confusing. (AP Photo/Eric Gay)
Friends and family watched her kids when they could during her treatment last year for colon cancer. But Davis had gaps with no help because she couldn’t afford child care and didn’t know where to look for assistance.
“I did not have the strength nor the energy to try to navigate these things myself,” the San Antonio, Texas, resident said.
Patients are not getting enough help dealing with a healthcare system that is growing increasingly complex, according to researchers and other experts in care delivery. They say more frequent insurance complications, doctor and drug shortages, and a lack of communication all make life harder for people with serious or chronic illnesses.
“Just about anything you can think of, it’s now harder to get it done, basically,” said Elisabeth Schuler, founder and president of Patient Navigator, a business that helps people get through the system.
More care providers and employers are offering help guiding people, a practice the federal Medicare program has started to cover. But that assistance has limits.
Patients with serious or chronic illnesses face a web of challenges. They include:
- Coordinating doctor appointments and tests, often while working or undergoing treatment.
- Dealing with coverage denials or care delays due to insurer pre-approval requirements.
- Figuring out how to fill a prescription if they can’t get coverage or their medication lands on a growing list of drugs in shortage.
- Acting as a go-between for doctors and specialists who don’t talk to each other.
- Paying medical bills and getting help with rent or utilities. That assistance has been harder to find since the COVID-19 pandemic, according to Beth Scott of the non-profit Patient Advocate Foundation.
All of this can be compounded for patients who don’t speak English or have no experience navigating the health care system, noted Gladys Arias, a policy principal with the American Cancer Society Cancer Action Network.
Davis, the San Antonio cancer patient, said she was in the hospital when she asked for help finding community resources.
She said a case manager set a book of available resources on her bedside table and did nothing else. Davis, a nursing professor, found the book confusing. The programs it detailed had different qualifications based on things like income or diagnosis. The 44-year-old wound up losing her car and leaving her home after care bills piled up.
“I feel like there was some type of help out there for me,” she said. “I just didn’t know where to look.”
Ali DiGiacomo said she wishes that she learned in college how to deal with insurance companies. She often has to do that while coping with side effects from rheumatoid arthritis treatments.
The 30-year-old personal trainer said she’s spent years trying to get a diagnosis for bouts of intense chest pain, which doctors think may be tied to her condition. That requires imaging tests that insurers often decline to cover.
“Dealing with them with brain fog and fatigue and being in pain is just like the cherry on top,” DiGiacomo said.
DiGiacomo said her formulary, or list of covered drugs, has changed three times. That can force her to hunt for a place that carries the newly covered drug, which puts her behind on her medication schedule.
She figures she talks to her insurer at least four times a month.
“I have to hype myself up,” she said. “Then you talk to a million different people. I wish I just had like one person that helped me deal with all this.”
Care delays due to insurer pre-approval requirements have grown more common, many experts say. More plans also have made it challenging to get coverage outside their networks of doctors and hospitals.
A typical appeal for a denial can easily involve 20 to 30 phone calls between the patient, the insurer and the doctor’s office, said Scott, director of case management for Patient Advocate Foundation, which helps people with chronic or debilitating illnesses.
She said some patients give up.
“Sometimes you are sick, and you don’t want to fight it anymore,” she said.
Case managers at hospitals are often overworked, which limits how much help they can provide, noted Schuler, who became a patient advocate about 20 years ago after her 2-year-old daughter went through cancer treatment.
Overall, help for patients is “very patchy everywhere,” according to Harvard Medical School researcher Michael Anne Kyle.
“I think we have a lot of Band-Aids that are necessary,” she said.
Many cancer centers offer patient navigators who can help coordinate appointments, get answers to coverage questions, find rides to the doctor and provide other support. Some insurers provide similar assistance.
And more employers are offering navigation or advocacy help for people on their insurance plans, according to the benefits consultant Mercer.
But these services still aren’t widespread. Alzheimer’s disease patients and their caregivers lack consistent access to such help, said Sam Fazio, a senior director with the non-profit Alzheimer’s Association.
“People are having trouble finding their way,” he said.
Making the system better for patients requires big change, said Dr. Victor Montori, a Mayo Clinic researcher who studies care delivery.
He said the system must focus more on minimally disruptive medicine, which makes care fit into patient lives. That means things like cutting unnecessary paperwork and surveys, making appointments more flexible and giving patients more time with doctors.
He noted that the burden that falls on patients is not just the time and effort they spend navigating the system. It’s also what they give up to do that.
“If you waste people’s time on silly things, you are being unkind to (their) main purpose, which is to live,” he said. “We have to stop thinking of the patient as a part time employee of the healthcare system that we don’t get to pay.”